| |
| |
| |
Welcome from Vicky and Annette | |
Welcome to this edition of the East Genomic Medical Service Alliance (GMSA) Nursing and Midwifery Genomics Newsletter. 22 March 2023 marks Lynch Syndrome Awareness day, so will that will be our focus in this edition.
Please share this newsletter with your colleagues and, if you haven't already, sign up to receive this newsletter here. | |
| |
Vicky Carr East GMSA Nurse Lead
Cambridge University Hospitals | | Annette Breen East GMSA Nurse Lead Nottingham University Hospitals | | | |
Funded Genomics and Counselling Skills Course | |
The University of the West of England is again running its popular online course, 15 credit module Genomics and Counselling Skills. This is open to all health care professionals. Apply for a funded place by Friday 21 April 2023 To find out more information click here | |
| |
| |
| |
| |
| |
- Bite Sized Genomics – Lynch Syndrome – Find Out More And ask Us Anything - Wednesday 26 April 12:45- 1:45. Register here
| |
Lynch Syndrome is an inherited cancer predisposition syndrome that makes people more likely to develop certain types of cancer. The chances that a person with Lynch Syndrome will develop specific cancers are higher than the general population:
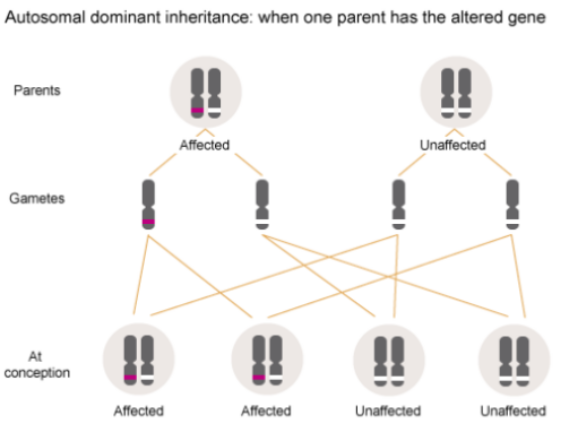
| Cancer | Lifetime chance of developing this cancer (general population) | Lifetime chance that a person with Lynch Syndrome has of developing this cancer | | Colorectal | 6 – 7% | 10 – 57% | | Endometrial | 3% | 13 - 49% | | Gastric | 1% | 13 - 19% | | Ovarian | 2% | 9 - 12% | | Brain/CNS | 1- 2% | 1– 3% | People with Lynch Syndrome also have a higher risk of developing biliary tract, pancreatic, urinary tract and skin cancers. Lynch Syndrome is caused by an alteration in one of five DNA mismatch repair genes; MLH1, MSH2, MSH6, PMS2 or EPCAM. These genes are important as they provide mechanisms to help protect against cancer by identifying cells that are unable to stop multiplying and repairing or removing them. It is likely that there are other genes related to Lynch Syndrome that aren’t fully understood yet It is an autosomal dominant condition, which means that 1 copy of an altered gene is needed for the condition to be present. If 1 parent has an alteration in any of these 5 DNA mismatch repair genes i.e. has Lynch Syndrome; there is a 1-in-2 (50%) chance that any child they conceive will have Lynch Syndrome. | |
| |
(Health Education England / Genomics Education Programme e-LfH) | | |
How common is Lynch Syndrome? It is estimated that 175,000 people in the UK are living with Lynch Syndrome: approximately 1 in 350 people have the condition. It causes over 1,100 colorectal cancers in the UK every year. Lynch Syndrome causes approximately 3% of colorectal and endometrial cancers.
How do people find out they have Lynch Syndrome? - Diagnostic testing: NICE recommends that all people diagnosed with colorectal or endometrial cancer should have molecular screening tests on their cancer. This is to find out if genetic testing for Lynch Syndrome is indicated.
- Predictive testing: People with a family history of Lynch Syndrome can have genetic testing known as “cascade” testing to find out if they have Lynch Syndrome.
Why is it important to find out if someone has Lynch Syndrome? - To plan the most effective chemotherapy for those with endometrial and colorectal cancers, and for those with colorectal cancer to inform how extensive their surgery should be.
- To diagnose cancers at an early stage when treatment outcomes are likely to be more effective, and may be less invasive to improve outcomes and quality of life. Lynch Syndrome means that people are at increased risk of developing certain cancers, and even if someone has had one cancer, they are at higher risk of developing another cancer in the same site or another site
- To agree a screening and management plan with the person including:
- Considering risk reduction surgery i.e. colectomy, hysterectomy, oophorectomy to reduce their risk of developing cancer in these sites
- Daily aspirin to reduce the risk of colorectal cancer
- Testing and treating Helicobacter pylori, a known risk factor for gastric cancer
- 2 yearly colonoscopy from the age of 25 or 35
- Reducing risk through lifestyle changes including stopping smoking, losing weight if obese, and daily supplements of resistant starch
| |
| |
Leanne is a parent and Brand Marketing Manager at Next, who lives with Lynch Syndrome...
Can you tell me when, and how you found out that you had Lynch Syndrome? In 2009, my Dad had a perforated bowel due to cancer; he had previously reported symptoms to his GP, which were not investigated further at the time, despite having previously had bladder cancer back in 2003. | | | |
He was very poorly and spent some time in intensive care, it was a long road to recovery but gratefully he’s now cancer free.
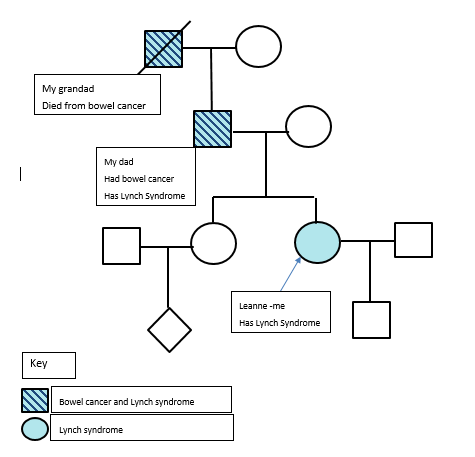
My paternal grandfather died of bowel cancer many years earlier, so we asked my Dad’s consultant if there was any link. The consultant was interested in family histories of bowel cancer, so my dad’s tumour was tested, and then he had genetic testing. The results showed that he has an alteration or mutation in his MSH2 gene, which means that he has Lynch Syndrome. The consultant recommended that my sister and I should have genetic counselling. We were referred to the Clinical Genetics service at UHL. The Clinical Genetics team were, and continue to be great; they took us under their wing and supported us to make informed choices about genetic testing. We both decided to go ahead with genetic testing. My result showed that I have the same gene mutation as my Dad so I have Lynch Syndrome, but my sister doesn’t. Here is my family history: | |
| |
What happened next? At that time, I was only 22, and wasn’t planning to have any children anytime soon. The Clinical Genetics Service supported me to make informed decisions about my surveillance programme, which means that I have regular scans for endometrial cancers and a colonoscopy every 2 years. When I first went for my colonoscopy appointments, I had to explain why I was there because I was so young. Because I have Lynch Syndrome, I am at higher risk of getting gastric cancer. I have also had screening for Helicobacter pylori, which is a risk factor for gastric cancer, which was negative.
Have you got any children now? Yes, I have a 5-year-old son, Jasper. I didn’t want my children to have to go through genetic testing and the 50-50 chance that they might have Lynch Syndrome. In 2015, I asked the Clinical Genetics team at UHL about pre-implantation genetic diagnosis (PGD) which is a procedure used in conjunction with IVF to reduce the risk of passing on some inherited conditions, including Lynch Syndrome. I was referred to Guys and St Thomas’ for this treatment. There were 4 embryos from our IVF; PGD showed that 2 of embryos were affected by Lynch Syndrome and 2 weren’t. In January 2017, I had one of the embryos implanted and later that year Jasper was born which I’ll be forever grateful for. It’s such a relief knowing that he won’t have to go through the worry of screening and genetic testing, and also that this will not affect his children going forward. We did want a brother or sister for Jasper, but unfortunately, the 2nd embryo failed to implant in 2020. How is your health now? Although I felt well, through the regular screening as part of the programme, there were some endometrial flags that were picked up towards the end of 2020. I made the decision to go ahead with an elective hysterectomy in February of this year to eliminate the risks associated with this. It was a decision that I didn’t take lightly but I wanted to ensure that I could have the healthiest future for me and my family and felt this was the best way. How has it affected the rest of your family? My Mum and Dad felt guilty because I inherited Lynch Syndrome, which was really hard for them. I’ve always tried to show them the positives in knowing about Lynch Syndrome and that I understand they weren’t aware of any of this when they had me. We told the rest of the wider family, some of them didn’t want testing and some did. Luckily, it appears nobody else has Lynch Syndrome that has been tested so far. Is there anything that you would like to say? I’m really grateful to you for reading my story and the rest of the information about Lynch Syndrome. I’ve previously met medical professionals that haven’t got an understanding of Lynch so it feels very supportive that people are taking their time to learn about this. | |
Meet Vicki Kiesel, Lead Genetic Counsellor | |
Vicki is Lead Genetic Counsellor, University Hospitals of Leicester NHS Trust and East Midlands Clinical Lead Lynch Syndrome...
Can you tell me about your role?
As a genetic counsellor, I see patients who are considering having genetic testing for many different conditions, including Lynch syndrome. | | | |
I discuss their medical and family history, and the implications of genetic testing. As well as the medical implications of Lynch Syndrome, we also discuss the psychosocial aspects of genetic testing.
For example, predictive genetic testing can be psychologically difficult so it is best not to arrange it at the same time it as major life events, such as exams. Genetic testing can also affect family dynamics. For example, 2 siblings may have different test results i.e. one may have a positive result and the other a negative result, so it is important to discuss how they may feel about this. In addition, to the implications for the patient, we also discuss the impact on future children and some people may choose to have PGD (pre implantation genetic diagnosis) so that their child doesn’t inherit Lynch Syndrome. I’m also the East Midlands Lynch Syndrome lead and as part of this role I’m helping to ensure that all endometrial and colorectal cancers are screened for Lynch Syndrome and that these results are incorporated into treatment management plans. We are also trying to develop mainstreaming pathways and set up a local Lynch Syndrome expert hub. What is mainstreaming Historically Lynch Syndrome genetic testing has been performed by genetic counsellors and geneticists as part of specialist clinical genetic services. However, for people diagnosed with cancer this means that they have to wait for a clinical genetics appointment appointment and this can delay their results. Mainstreaming aims to support healthcare professionals within the MDT (multi-disciplinary team) to explain and order genetic testing, meaning that patients don’t need to be referred to clinical genetics for testing which hopefully speeds up access to their results. Mainstreaming ambitions 95% of people with Lynch Syndrome don’t know they have it. which means they don’t have access to screening and other risk reducing options. The National Lynch Transformational project and mainstreaming hopes to identify more people with Lynch syndrome, meaning that they and their relatives can have access to genetic testing and appropriate screening. We hope this will decrease the number of cancers diagnosed and mean that they are diagnosed at an earlier stage. We hope that all hospitals will help to embed Lynch Syndrome testing within their cancer diagnostic services to enable the prevention of, and early detection of Lynch related cancers. Lynch Syndrome Hub The Lynch Syndrome hub will coordinate care for people with Lynch syndrome ensuring that they have access to the most appropriate screening and expertise. | |
Meet Professor Julian Barwell | |
Julian is a Consultant Cancer Geneticist at UHL and Professor in Genomic Medicine, University of Leicester who is developing an App for Lynch Syndrome patients...
Can you tell me more about the difficulties that Lynch Syndrome patients face? In Leanne’s article above, she says, “I’ve previously met medical professionals that haven’t got an understanding of Lynch…” and many of our Lynch Syndrome patients have this experience too. | | | |
This means that they often struggle to access timely information, advice and support for their care. | |
Can you tell me more about the App and why it will be helpful?
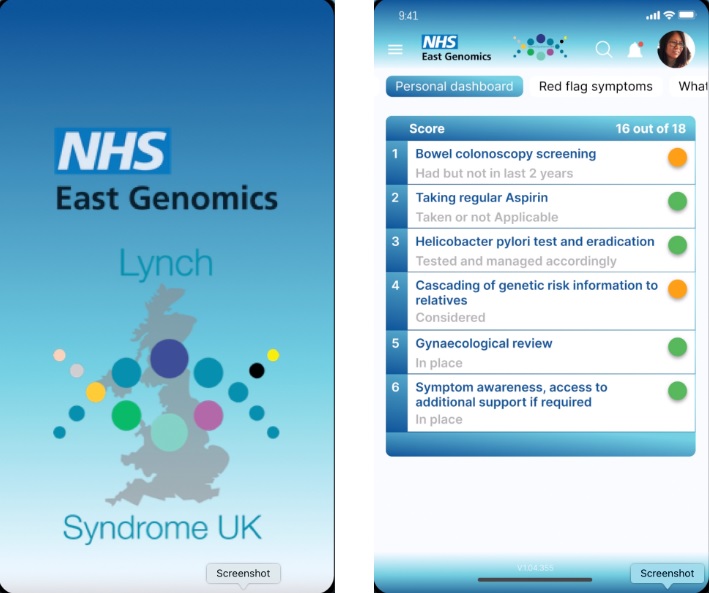
I am leading a project in collaboration with Instant Access Medical Ltd to develop a mobile phone App. This will empower patients to deal with health care professionals and enable them to participate directly in their care to prevent complications, personalise their health and well-being plans, and improve their outcomes. The project is supported and co-developed by Lynch Syndrome patient champions and Lynch Syndrome UK, and is informed by patient questionnaires through IPSOS-MORI, the global market research company. The aim is that, on completion of the pilot, the App will be rolled out nationally for all carriers of Lynch Syndrome to help them navigate the NHS on a day-to-day basis. Will it be launched soon? We are hoping to launch the App for Lynch Syndrome patients at the UHL Clinical Genetics Service over the next month or two. The App will be rolled out in a phased way: - Do Lynch Syndrome patients download it and use it? How do they feel about it?
- Expand the App to include red flag symptoms
- Roll the App out more widely
- Link to NHS systems with reminders for colonoscopies, etc
We will evaluate at each stage carefully using IPSOS-MORI before progressing. The final stages will be to include dihydropyrimidine dehydrogenase (DPYD) gene testing; this is to increase the safety of chemotherapy for cancer patients, and then we hope to develop Apps for patients with other genetic conditions | |
| |
Mainstreaming in Practice | |
Kirstie Williams, Gynae Oncology Clinical Nurse Specialist, Nottingham University Hospitals NHS Trust (NUH)... Can you tell me about your role?
I see patients in clinic to support them with their choices about treatment and care and manage complex, individual and changing information and support needs of patients throughout their whole gynae cancer care pathway, see patients when they are told that they need surgery, post operatively for results and then for their follow up appointments.
| | | |
I attend gynae cancer MDT meetings where patient diagnoses and treatment plans are discussed. The CNS role at this meeting is to act as the patient advocate, and contribute to the meeting any relevant information we may have following conversations with the patient.
The CNS team also support patients and counsel them at their pre-operative assessment appointment, ensuring they have all the necessary information regarding their planned surgery.
I also run nurse led follow up clinic with my colleague Cat Warren. This is for low risk early stage endometrial cancers (Grade 1-2, Stage 1a). At this appointment, we complete a holistic patient needs assessment and if required a vaginal examination.
Can you tell me what mainstream genomic testing means for patients in your service? GPs and some other specialities refer symptomatic patients to gynaecology clinics for assessment under the 2-week wait. This assessment decides whether the patient needs a biopsy / hysteroscopy. At our weekly gynae cancer MDT meetings, we review all laboratory results of each patient’s biopsy / hysteroscopy which includes a review of the DNA mismatch repair protein results in the tumour. If one of these proteins is missing from the tumour, it means that the patient is at risk of having Lynch Syndrome. We changed our MDT patient proformas so that they include a question or prompt about genomics, which helps our failsafe processes for each patient. We sometimes get patients referred to our service from other hospitals after their biopsy; and their biopsy hasn’t had laboratory testing for the DNA mismatch repair proteins. We follow this up to ensure that these tests are completed. At the patient’s next appointment with a clinician and CNS; their results, treatment options and genomic testing are discussed. CNSs offer genetic counselling to patients whose results show that 1 or more of the DNA mismatch repair proteins are missing from their tumour. This involves a detailed discussion with the patient, as there is a lot of complex and potentially distressing information to go through; including that the test results might show that they are risk of having other cancers in the future, and that if the genetic result is positive their family members might have inherited the gene alteration which means that they at higher risk of developing cancers. This is hard when they’ve just been told that they have endometrial cancer, I really feel for them. The genetic test results are reviewed by our Lead Gynae Cancer Genomics Consultant. Patients with a positive or non –informative genetic test result are referred to Clinical Genetics for more detailed, specialist genetic counselling How do patients feel about being offered genomic testing by your service? The patients find it helpful that they are offered genetic counselling and testing at the same appointment as it means that they don’t have to come back for more appointments. From the consents I have taken, I have had no one who has refused genetic testing so far. I do think that they have a lot of information to take in at that appointment including consenting for treatments and all the implications of that What education and training did you have? The Clinical Genetic Services at NUH supported us with bespoke education and training for our role. And it’s fantastic that we have strong links with them so we can ask for their help and advice with more complex cases How do you feel about your role in mainstreaming genomics? It was quite daunting to begin with, but now I think it’s really positive that it’s become part of our routine patient care pathway and that we as CNSs have such a key role. It’s great that that our patients don’t have to be referred and wait for a separate appointment for genomic testing. | |
Where can I find out more information? | |
| |
Meet the East GMSA Nursing and Midwifery Team | |
| |
| |
Education, Training and Resources | |
| |
| |
| |
| |
| |
If you would like to unsubscribe to these newsletters please email us | |










.jpg)
