| | | | | | | | Welcome from Vicky, Annette and Jo | | Welcome to the November 2023 edition of the East Genomic Medical Service Alliance (GMSA) Nursing and Midwifery Genomics Newsletter. In this edition, we focus on cancer genomics and our United Against Prostate Cancer project.
And it’s “Welcome” from Vicky for the last time as we say “Goodbye for now” as she is leaving us to start her new role as Head of Accreditation and Harm Free Care at Cambridge University Hospitals NHS Foundation Trust. Thank you Vicky for all your hard work with us, we really appreciate it. I’m sure that you’ll join us in wishing Vicky all the best in her new role.
Please do share this newsletter with colleagues and encourage them to sign up to receive it here. | | | | Vicky Carr East GMSA Nurse Lead
Cambridge University Hospitals | | Annette Breen East GMSA Nurse Lead Nottingham University Hospitals | | Joanne Hargrave East GMSA Midwife Lead Norfolk and Norwich University Hopsitals | | | | | | Meet María Echevarría Gutiérrez, Genetic Counsellor - United Against Prostate Cancer, University Hospitals of Leicester NHS Trust (UHL)
What is your role? I am a genetic counsellor and our role is helping patients and families who have a genetic condition or who are at risk of having a genetic condition. | | | | Every appointment is different, as every patient has their own personal needs and concerns. Our range of responsibilities may include assessing our patients’ risk of developing a genetic condition, how this condition may impact them and/or their family, helping them understand their options and implications for genetic testing (including risks and benefits) and providing them with the best information and support to help them make decisions. If a patient decides to have genetic testing, we discuss their personal results and how this can affect them and other family members. During our appointments, we try to give patients individualised support according to their needs and family situation and provide them with resources and further help if required.
Tell us about the Clinical Genetics service There are 15 Clinical Genetics services across England. Each service covers an area with a population of between 1 and 5 million people.
I am based at the Leicestershire Clinical Genetics Service which is coordinated through our base at UHL and we do regular clinics in other hospitals across Leicester, Leicestershire, Northamptonshire and Rutland. We have consultant geneticists, registrars, genetic counsellors and nurses, research and project nurses and an admin team. Genetic conditions can affect any body system and we see patients of all ages to diagnose genetic conditions, and / or asses the risk that they will inherit or develop a genetic condition.
Can you us a little bit more about cancer and genomics? All cancers are genetic, they develop because there is a variation or something has gone wrong with one or more of the genes in a cell. Most cancers are sporadic with environmental causes. In other words not inherited, and are diagnosed later in life. However, 5% to 10% of cancers are hereditary. Therefore, we can see that a complex mix of genetic, lifestyle and environmental factors during our lives influences our personal risk of developing cancer. | | | | What might suggest that someone is at risk of an inherited cancer? They have a large number of relatives on the same side of their family diagnosed with cancers at an earlier than average age - below the age of 50. Either they or one of their relatives has or had multiple tumours e.g. bilateral breast cancers, breast and ovarian cancers, multiple bowel cancers. Or there are clusters of different cancers in a recognisable pattern in their family. When we talk about relatives here, we mean first or second degree relatives.
We also think about ethnic origin. For example, breast cancer is less common in those of Indian or Chinese origin, so any family history may be more significant.
Why are people with inherited cancer predisposition genes at higher risk of developing cancer? Because they have inherited a variant in either their: - DNA repair genes which maintain the integrity of the genome by repairing DNA damage, or
- Tumour suppressor genes which inhibit cell production, or
- Proto-oncogenes which promote specialisation and division of normal cells
What types of cancer predisposition syndrome are there? There are more than 200 cancer predisposition syndromes. Each of these syndromes is quite rare; here are a few examples: - Breast – BRCA1, BRCA2, PALB2, CHEK2, Li Fraumeni
- Bowel – Lynch, Familial Adenomatous Polyposis
- Renal – Birt Hogg Dube
- Endocrine - Multiple Endocrine Neoplasia
What types of cancer genomic tests are there?
In Clinical Genetics, we see patients to find out if they have an inherited gene variant, which increases their risk of developing cancer. These gene variants occur in the sperm or egg cell and are passed directly from parent to child at the time of conception and are then present in every cell in the body. There are two types of testing: - Diagnostic testing: looks for the gene variant. Completed on a blood or tissue sample from someone in the family who has been affected with the cancer.
- Predictive testing: if diagnostic testing finds a gene variant, other family members can be tested for the same variant.
Personalised medicine is looking at developing treatments to target the genetic make-up of a cancer. There are different gene variants in different cancers and each person’s cancer has its own individual genetic make-up; personalised treatment aims to target these differences more accurately so that patients can have the most effective and safe treatment for them as an individual. These gene variants are somatic or acquired from damage to the genes in an individual cell or cells during a person’s lifetime.
Jo and Eddie [below] talk about our United Against Prostate Cancer project which draws these two different types of testing together.
To summarise, why is cancer genomics important? It’s really important to find out if a patient has a cancer predisposition syndrome because: - it may change their treatment plan, for example targeted chemo or immunotherapy
- they are at risk of developing cancer if they have never had cancer, or of developing another cancer if they have already had cancer. This means that they can be offered screening or other interventions to help improve the chances of an earlier diagnosis, chemoprevention and prophylactic surgery where applicable
- they may be able to make informed decisions about their reproductive choices, for example pre-implantation genetic testing may be possible for a few
| | | | Meet Jo Lowry, Regional Programme Manager for the East Genomic Medicine Service Alliance (GMSA)
What is the United Against Prostate Cancer project? It’s a pilot project to tackle prostate cancer disparities, linking educational, clinical and laboratory capability with outreach, insight and support to improve awareness and access to services. | | | | We are exploring ways to improve the prostate cancer-testing pathway through sustainable transformation for genomics across the East GMSA region. We're working with clinical and scientific colleagues, stakeholder partnerships and community champions to tackle health inequalities and inequities surrounding prostate cancer. Our aim is to improve the care of men and support for their families by improving awareness of prostate cancer and genetic testing within high-risk groups, individuals with a relevant family history and/or of an African / African Caribbean heritage.
This is part of a national pilot to establish genetic testing of prostate tumour tissue samples to help identify the causes of this disease in patients. This could be useful in planning their treatment, moving to personalised medicine, or determining if their relatives could also be at an increased risk of breast, ovarian or prostate cancer, through diagnostic testing to look for a gene variant.
Why Prostate Cancer? There are over 52,000 cases of prostate cancer every year in the UK and it accounts for 27% of all male cancers. It affects 1-in-8 men during their lifetime; this risk increases to 1-in-4 for men of African / African Caribbean heritage. As well as being at higher risk, the death rate for men of African / African Caribbean heritage with prostate cancer is 30% higher than for white men with it. Men with a first degree relative, a brother or their father, who had prostate cancer are also at higher risk. 5 year survival rates vary depending on the stage that prostate cancer is diagnosed at. Almost 100% of those diagnosed at Stage 1 or 2 will survive for 5 years or more compared to 50% of those diagnosed at Stage 4. For more information see Cancer incidence for common cancers | Cancer Research UK and Hear Me Now! The uncomfortable reality of prostate cancer in African Caribbean men - Download Summary - BMECC
What is East GMSA doing? There are a lot of different things that we have been working on: - Enabling a stakeholder group to support families in need
- Establishing genomic tests in the NHS Genomic Test Directory
- Developing communication and strategic planning across stakeholders
- Enriching insight into healthcare from members of our community
- Emotional support to each other at a difficult time to enact care
- Enabling early diagnostics for high risk through additional equipment and resources to support genomic investigations
- Working with commissioners and commercial groups
- Encouraging stakeholder group leadership
- Educating healthcare professionals on new developments
- Ensuring equity across the East GMSA geography
We’ve been involved in and hosted lots of community and engagement events across the region including ‘Play Domino, Talk Prostate’ events, a Lord Mayor endorsed collaborative event at the Leicester City Football Club and linked with esteemed dignitaries, celebrities and the Arts as a lever of engagement.
In June, Maria, Councillor George Cole and I were guest sponsors at the Nottingham Arts Theatre production of One-In-Four which tackled head on the fears that some black men have towards getting tested for prostate cancer. Our team has done radio interviews, attended the Leicester African Caribbean Cup Football Tournament Community Cup to support the 75th Anniversary of the Windrush generation, presented at golf club events and much more - a snapshot of this work is captured in the image below.
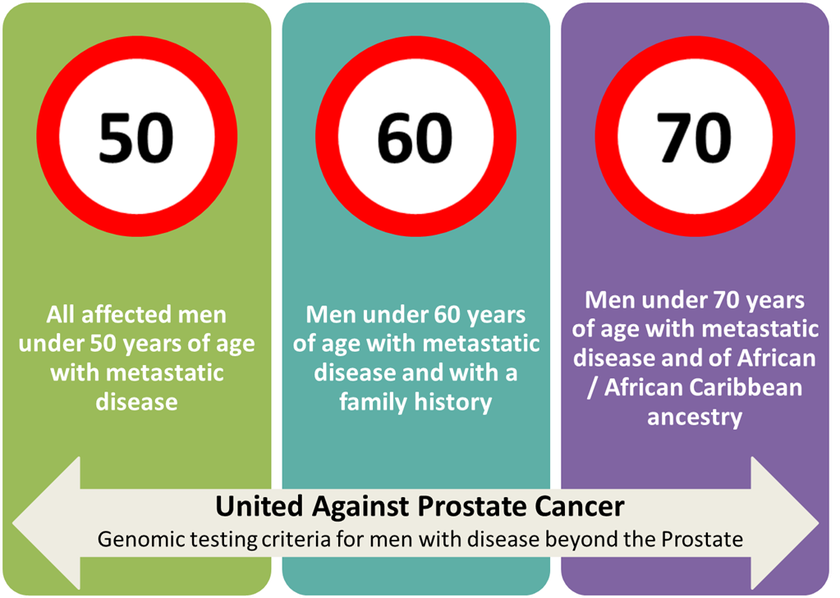
| | | | Who is being offered testing? Since April 2022 as part of the project pilot somatic testing pathway, we have offered testing across the East GMSA region for: - all affected men <50 years of age
- those <60 years of age with a family history
- those <70 years of age of African / African Caribbean ancestry with metastatic disease
| | | | Things have now moved on, as genomic testing is more widely available and commissioned by the NHS: for men with either: - Prostate cancer diagnosed <50, or
- Metastatic prostate cancer diagnosed <60, or
- Ashkenazi Jewish ancestry and prostate cancer at any age, or
- 10% chance of a genetic mutation.
This year, personalised or targeted medicine took a step forward when NICE recommended olaparib for those with metastatic castrate resistant prostate cancer. The National Genomic Test Directory for rare and inherited disease was also updated to include test number R444.2 (NICE approved PARP inhibitor treatment for prostate cancer, which is indicated if somatic testing for prostate cancer, test number M218.1 has failed).
Olaparib is a poly adenosine diphosphate-ribose polymerase (PARP) inhibitor. PARP is an enzyme that helps cells repair damaged DNA. By blocking this enzyme, PARP inhibitors prevent the DNA of cancer cells being repaired, preventing them from growing and spreading while leaving healthy cells much less affected.
It's great news that there is progress on our project aims, but we’re still working hard to achieve equitable access for this, and all genomic testing across the East GMSA region. | | | | Meet Eddie Blair, entrepreneurial scientist, cyclist, walker, golfer, gym goer and more…and living with prostate cancer.
When, and how did you find out that you had prostate cancer? When I went for my routine NHS Health Check in August 2022, there was some glucose in my urine so the practice nurse did an HbA1c blood test. | | | |
I asked the if I could have a PSA (prostate specific antigen) test at the same time and she advised me to see the GP to discuss the implications and limitations of it, which I did. The GP found that my prostate “was moderately enlarged”. I didn’t really have any symptoms; just bit of back ache which I put down to playing golf badly, and I was getting up in the night to go to the toilet, which I put down to having a beer or two.
On 15 September, my PSA test results were were >600 ug /l (normal range is 2.5ug/l – 6.5ug/l) suggesting advanced prostate cancer. During the next few weeks, I had prostate biopsies, CT cans, bone scans and more PSA blood tests. On 11 October, I was told that I had stage 4 metastatic prostate cancer; it had spread to many of my bones and some lymph nodes too.
What happened next? My treatment started on 22 September with an androgen deprivation therapy (ADT) called bicalutamide and two weeks later, my PSA level was down to 371 ng/l. Then I started on decapeptyl, a gonadotropin releasing hormone agonist, to lower my testosterone levels. Towards, the end of October, my PSA levels were down to 279 ng/l.
My ADTs since then have changed to daily enzalutamide and three-monthly goserelin, which I am still taking with no major side-effects, except loss of libido. At the beginning of November, my bone density was normal and I was asked if I would be willing to have further testing on my biopsy tissue. I consented, as I’m very keen to have any genomic testing and join any appropriate clinical trials. I also gave blood for DNA testing which showed that hereditary cancer markers, such as BRCA1 and BRCA2, were absent which was great relief to my kids, my siblings and their kids.
Where does genomic testing fit in? I joined the East GMSA Patient and Public Voice Panel and at a face-to-face meeting got talking to Jo Lowry and Gemma Gunn who were working on the United Against Prostate Cancer (UAPC) Project. I was very interested and wanted to enrol. My biopsy tissue underwent genomic testing to look for alterations in 17 genes in the cancer cells. Thankfully there were no alterations in 16 of them including BRCA and a few others, which means that my cancer is unlikely to be hereditary and have implications for my family – phew! There was a BRAF gene alteration (BRAF genes promote specialisation and division of normal cells), which probably explains why although I had advanced prostate cancer I didn’t really have any symptoms. But good news, the gene alteration is limited to my prostate cancer only and shouldn’t affect other parts of my body. And more good news, this meant that my treatments could be more precisely targeted to my specific cancer and indeed, I am enrolled in precision medicine research trials at the Royal Marsden.
How is your health now? All things considered, fantastic. Although my PSA levels are starting to rise from 5ug/l to 17ug/l – probably an indication of limited tumour resistance to current ADT! However, my bone scans show continued improvement in my bone mets and no new ones, and my most recent CT scan shows that lymph node involvement is diminished! I’m keeping up with golf, cycling, gym, yoga and gardening and have just been on a walking holiday to the Lake District, conquering some of the “Wainwrights” (peaks or fells above 300m). I was told that I would never be cured of cancer, but now I’m living with it and will die with it rather than from it. Last year, The Institute of Cancer Research announced that it should be able to cure advanced cancers within the next 10 years by targeting the tumour microenvironment, and cures through immunotherapy and targeted therapy have been reported in the last few weeks so I’m optimistic and under the care of the amazing uro-oncology team at Addenbrooke’s and East Genomics. Indeed several clinical colleagues have said “See you in 10 years!” which can’t be bad. Find out more:
| | Genomics BITE: Cancer Genomics | | | | For those of you working in cancer care and urology (and anyone who is interested in finding out more) our next Genomics BITE session will focus on Cancer Genomics and The United Against Prostate Cancer Project and takes place on Wednesday 15 November, 12:30pm – 1:45pm via MS Teams. Register for your place here.
You can watch our previous Nursing and Midwifery Genomics BITE sessions on our Project resources and outputs webpage here. | | | | | |
You can now register (click to proceed past the warning message) for this year’s NHS Genomics Healthcare Summit, taking place Tuesday 12 December at The Kia Oval, London. The programme will include plenaries covering what has been achieved since last year’s inaugural summit which featured the launch of the Accelerating genomic medicine in the NHS strategy; ongoing work to mainstream genomic medicine in the NHS; how alignment with research is driving improvements in patient care and a look towards the future with genomics embedded in the NHS. There will also be a range of workshops exploring, among other things, the role and impact of patient and public involvement in the NHS GMS, the evolving Clinical Genomics Service model, the use of data to address health inequalities in NHS genomics and further efforts to support the NHS workforce to deliver timely and effective care. The full agenda will be added to the website soon. | | | |
Monogenic Diabetes Virtual Training Course 6 and 7 December 2023 This 2-day virtual course is aimed at Diabetic Specialist Nurses and Midwives, consultants and SpRs to help recognise and treat patients with MODY and other types of monogenic diabetes. Find out more and book your place here. | | | |
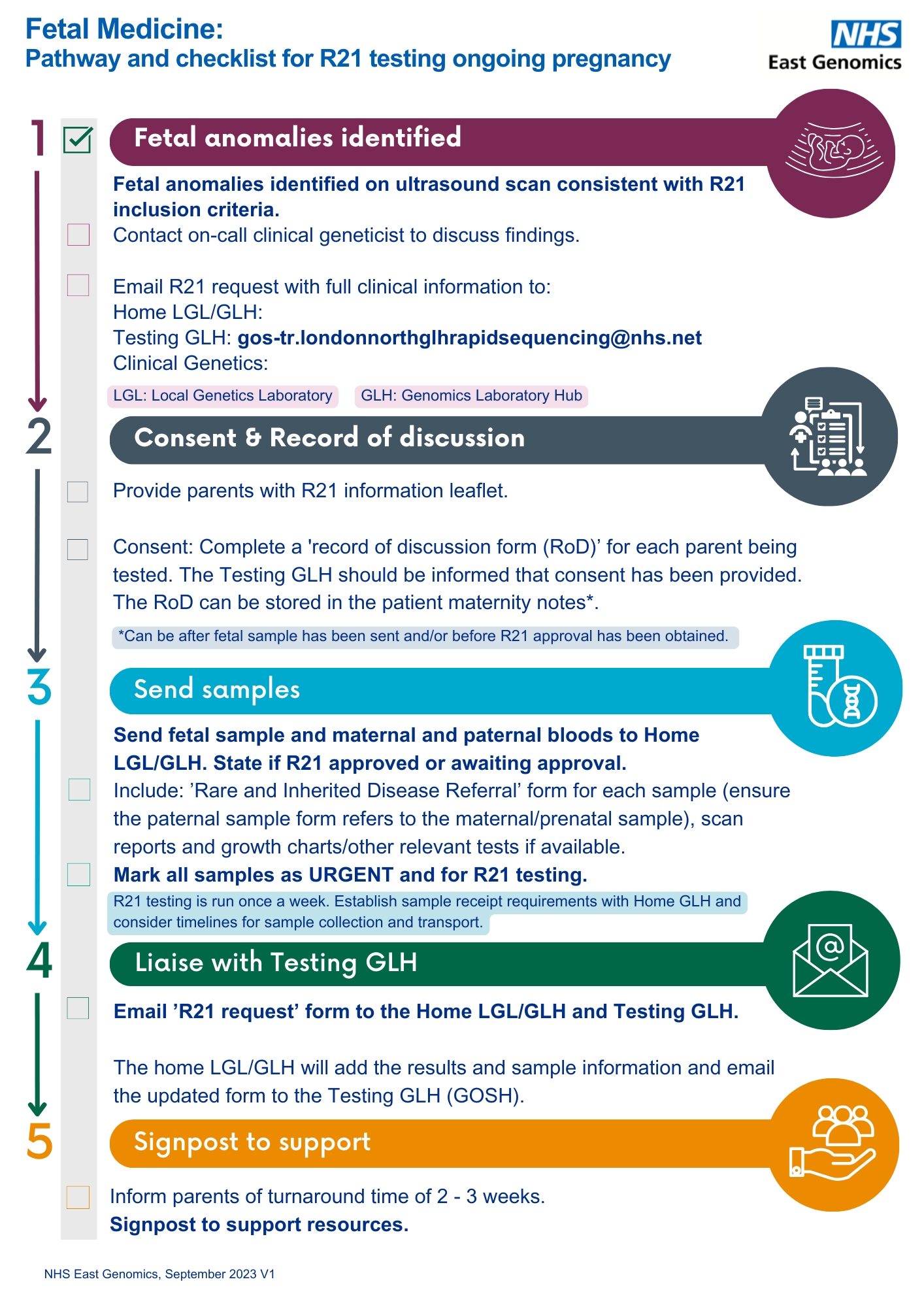
East GMSA R21 final project presentation Tuesday 7 November 2023 10.00am – 11.30am via Teams This session is aimed at doctors, midwives and allied health professionals who are currently working within prenatal pathways. Further details of the event and joining instructions can be accessed here and we would be grateful if you could share this invitation with your colleagues and networks. Our R21 test directory quick user guide and workflow documents are now available for you to access on the East Genomics website. We have also uploaded a recording of the recent R21 lunch and learn session to our project webpage. | | | | | |
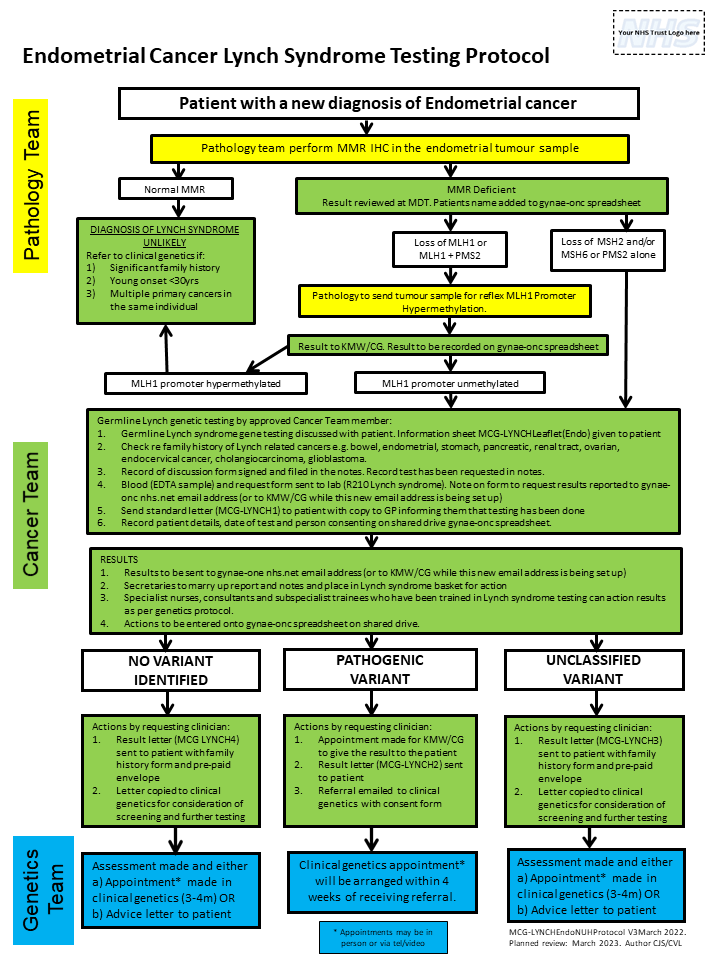
Generation Study The Generation Study is an NHS-embedded research study which aims to understand whether sequencing babies’ genomes can help to discover rare genetic conditions earlier. It aims to look at the DNA of over 100,000 babies and gather evidence to consider whether whole genome sequencing could be rolled out as part of a future newborn screening programme. It is estimated that the study will identify suspected diagnoses for between 500 and 1,000 of the 100,000 babies that take part in the study. Genomics England published their initial list of over 200 rare conditions that will be looked for as part of the Generation Study at the beginning of October. This initial list may be subject to change during the study to add or remove condition as research and evidence emerges. | | | | Lynch syndrome patient event and East Midlands Lynch Syndrome Expert Network (EMLSEN) launch On Wednesday13 September we co-hosted a Lynch syndrome (LS) patient event in Leicester with East Midlands Cancer Alliance.
We also took the opportunity to officially launch the new East Midlands Lynch Syndrome Expert Network. | | | | Patients joined us to get information and support, and enjoyed talks on health management of LS, speaking to children and relatives about LS, LS and the menopause, prostate cancer screening and talks from fellow LS patients. The new East Midlands Lynch Syndrome Expert Network (EMLSEN) is an expert MDT which provides expert, equitable care for those with Lynch Syndrome across the East Midlands. Clinicians can refer their LS diagnosed patients into EMLSEN. Find out more, including how to refer you patients here. Check our website over the coming month for more information on the new East of England Lynch Syndrome Expert Network (EoELSEN). | | | | East GMSA project resources and outputs A number of East GMSA projects are producing outputs which are being added to the East Genomics website. Our Feto Maternal Genomic Pathways project team have added a new resource page containing an R21 testing inclusion/ exclusion criteria poster and a Pathway checklist document.
Our Cystic Renal Disease project team have added two poster infographics - one aimed at healthcare staff and the other at patients and the public. Please see our webpage here for more information about how to use these resources in your service. | | | | | | Regional Lynch syndrome Nurse, Melissa, at 7th annual European Hereditary Tumour Group meeting The National Lead Nurse for the Lynch Syndrome Project and some of the Regional Lynch Syndrome Nurses attended this meeting in Vilnius, Lithuania last month.
Presentations were given by: | | | | - Amy (North East & Yorkshire GMSA) - The National Nursing Workshops: Adapting Delivery and Content to Increase Awareness of Lynch Syndrome
- Mandy (North West GMSA) & Melissa (East GMSA) - The United Kingdom National NHS Genomic Lynch Syndrome Transformation Project: The Rise of the Genomic Practitioner
- Anna (North Thames GMSA) - Setting up the Regional Lynch Syndrome Expert Network for the North Thames GMSA
- Siobhan (South West GMSA) - Confident to mainstream genomic testing in Lynch Syndrome? A competency guide for nurses
- Laura (National Lead Nurse) - The UK model for mainstreaming in Lynch Syndrome
There was also the launch of the EHTG European Nursing Network for Nurses that provides services for Lynch Syndrome patients with representation from the UK, Ireland, Spain and Italy and included nurses, charities and patient representatives.
The EHTG focuses on prevention, diagnosis and treatment of hereditary tumour syndromes and is proud to host the PLSD (prospective lynch syndrome database). | | Education, Training and Resources | | The Genomics Education Programme has a wide range of free to access learning and education resources for nurses, midwives and health visitors. No matter where you are in your leaning journey about genomics, there is something for you to build your knowledge and support your NMC revalidation including: - Bite size genomics a series of 10 minute animations and films
- Genomics 101 a series of 9 short introductory courses, each lasting about 30 minutes for those with a little bit or no knowledge about genomics
- Taught courses up to Masters level
- GeNotes help healthcare professionals make the right genomics decisions at each stage of a clinical pathway. GeNotes are in development to provide:
- In The Clinic information focussed at the point of patient care with clinical scenarios, when to consider genomic testing, what you need to do and the results stage
- A Knowledge Hub accessed via links within ‘In The Clinic’ to external sources and resources and signpost to relevant guidelines, including NICE.
| | Meet the East GMSA Nursing and Midwifery Team | | | | | | | | | | | | | | If you would like to unsubscribe to these newsletters please email us | | | | | |











.png)

_(1).png)

.png)

.png)