I am based at Guy’s and St Thomas’ NHS Foundation Trust to help collaborate with Trusts across the South East region to establish mainstreaming, i.e., develop renal genomic pathways and incorporate genetic testing as part of the clinical toolkit for kidney disease management.
We have engaged a few key Trusts and are currently expanding throughout the region and across other GMSAs to develop and support clinical genetic pathways and overall promote national equity of access.
We have followed a model to implement our ‘Think DNA, Think Genetics’ initiative by engaging in academic meetings with nephrologists, linking with practice development nurses and midwives and managers to introduce, develop, educate and upskill healthcare professionals. Specifically through tailored study days, ‘Lunch and Learn’ webinars and by working closely with renal nurse educators at London South Bank University, Kings College and St George’s/Kingston University and contributing to their postgraduate certificate renal nursing modules.
This is furthered by the support of the Association of Nephrology Nurses UK (ANN-UK) to improve delivery across the national professional group. My ambition is to help develop and integrate more nurses, midwives & allied healthcare professionals through education and upskilling to become genomic champions to support their local clinical kidney team to improve patient benefit.
We have incorporated a nurse-led renal genetics clinic (Guy’s Hospital) to coordinate care pathways in partnership with nephrologists and aim to include the advances in genomic medicine for kidney patients across their whole pathway. For the patients I see I want to help reduce their patient ‘diagnostic odyssey’ through genetic testing and improve tailored renal care (precision medicine, transplantation decisions, family testing, pre-implantation genetic diagnosis, counselling). The team also provides further support to Trusts in the South East to develop their own local kidney genetics clinics.
Most importantly, we work closely with Patient Public Involvement (PPI) groups including the Polycystic Kidney Disease Charity, Nephrotic Syndrome Trust and Alport’s Society Foundation. We are keen to engage with more PPI groups to empower patients, support in the planning, delivery and evaluation of renal genomic pathways.
"In less than a year, there has been a 111% increase in uptake of renal (kidney) genetic testing across the South East region".
.
Can you tell us about a patient for whom genomic / genetic testing has proved life saving?
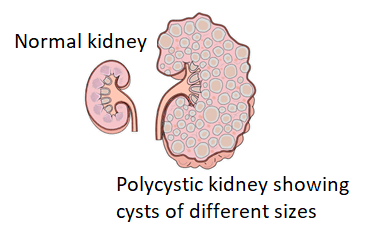
At 6 months old, baby B had no urine output, end stage kidney failure and had started kidney dialysis. Baby B’s ultrasound scan showed multiple renal cysts and the initial diagnosis was autosomal recessive polycystic kidney disease (ARPKD). Baby B also had low serum albumin, which was thought to be due to sepsis. A kidney biopsy was ruled out because it was unlikely to add any additional information to the diagnosis and because Baby B was too young.
Baby B had genomic/genetic testing which showed that they had Denys-Drash syndrome, which causes kidney failure, genital anomalies and Wilm’s tumour, a rare type of kidney cancer that affects children. Genomic/ genetic testing meant that Baby B had an accurate diagnosis, which changed their care and treatment pathway. Baby B then had both kidneys removed and the tumours had not spread beyond their kidneys.
What is the most rewarding thing about your job?
Positive patient feedback and enhanced patient-centred care. The potential to delay and/or even prevent progressive end stage kidney disease, enhance informed decision in live-donor transplantation, improve surveillance, genomic counselling, family planning (pre-implantation genetic diagnosis) and to improve equity of access and collect meaningful data which demonstrate the positive impact that genomics is having.
What is the most challenging thing about your job?
The demands on the NHS and staff shortages means that there are different levels of engagement and support from each of the NHS Trusts that I work with. Currently many nurses, midwives and clinicians are not fully prepared to integrate genetic/genomic health information into their everyday clinical practice. This means that patients and their families may not have the benefit of genetics/genomics to inform their care and treatment pathways and decision making.
The 7 GMSAs across England are working to engage stakeholders to build and develop the current and future workforce to incorporate genetics/genomics into their everyday clinical practice. This is essential to realise the benefits that precision medicine can bring to kidney care pathways.
I am passionate that all kidney patients should have equitable access to renal genomic pathways, so I will continue collaborating across the South East region and through other GMS-Alliances.








")